Equine Spinal Fractures Causing Neurological Signs
Equine Spinal Trauma Fractures, Signs, and Symptoms
Your horse may have suffered from a fall or a hit to the head or neck, resulting in a spinal fracture. This spinal fracture usually has an acute onset and a history of trauma. Trauma fractures display neurological signs and symptoms, including seizures, ataxic behavior, inability to get sternal or stand, dilated pupil, and blindness. The trauma fractures discussed here are concerning the Skull, Cervical spine, Thoracic spine, Lumbar Spine, and Sacrum/Coccygeal. Also included is a discussion of Spinal Stenosis and Stylohyoid Osteoarthropathy.
Skull Fracture
Fracture of the skull usually has an acute onset and a history of some form of trauma. A direct blow by a kick or an object such as a fence, pipe stock, etc. Horses that fall over backward (flippers) and strike the top of the skull (external occipital protuberance) often have loss of consciousness with mild to severe seizures and hemorrhage from the external ear and/or Nares.
If they are able to stand, they are obviously displaying at least Grade 3 ataxic behavior with a head tilt (torticollis) strabismus (unilateral or bilateral) nystagmus and many times are visually blind as the countercoup fracture associated with this trauma can either directly traumatize the optic nerve or the hemorrhage into the tight compartment in the Circle of Willis puts pressure on the optic nerve which results in dysfunction. An ophthalmologic exam will usually disclose a dilated pupil, lack of menace, normal eyelid tone, and swelling of the optic nerve.
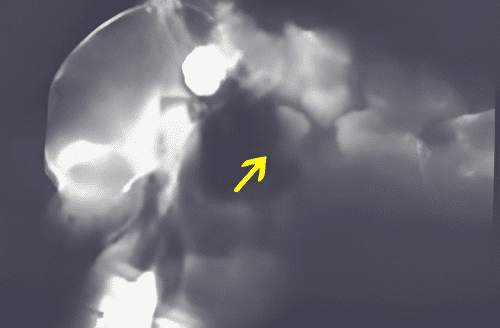
If the patient is stable, then standing pharyngeal films will show the guttural pouch to be filled with fluid (hemorrhage) instead of air. The prognosis depends on the response to time and anti-inflammatory medication. If there is still blindness after 30 days with a dilated pupil and atrophy of the optic disc, the prognosis for performance is poor.
Cervical Spine Fracture
Fractures of the cervical spine usually have a history of trauma with an acute onset. Falling on the cervical area while jumping, pulling back when tied to an inanimate object, or running into a stout fence with the head extended are characteristic histories. They may also present as colic, as the pain and discomfort are very obvious. Foals with Salter fractures of the cervical body endplates have a dramatic ventral distortion of the mid-cervical area. If the patient is in lateral recumbency and cannot become sternal or stand, then a fracture of the lower cervical bodies with severe cord compression should be considered.
Radiography is indicated to assist in the diagnosis. Initial treatment is the standard anti-inflammatory medication previously mentioned. They should be offered feed and water in an elevated (chest-high) position. The degree of ataxic behavior will improve rapidly in most cases. If the patient is still standing and radiographs show a fracture, additional imaging such as CT scans and myelography are not indicated unless the degree of ataxia does not improve or becomes more dramatic. Often, the articulation anterior or posterior to the fracture causes cervical stenosis. The majority of cases do improve and either return to competition or, in the case of a foal, develop into performance horses.
Thoracic Spine Fracture
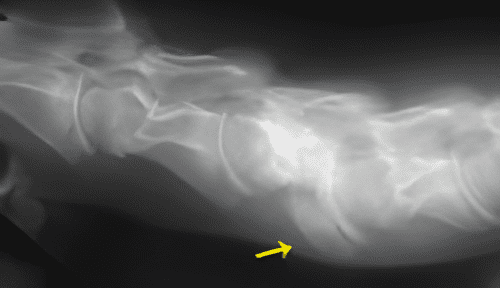
Trauma to the thoracic spine is usually a result of falling over backward and directly striking the dorsal spines or being trapped beneath very stout objects and trying to rise (a pipe restraining stock). Fractures of the dorsal spine usually are from T4- T8, and there is marked deformity (flattened withers) and swelling. There is local pain, and the patient does not want to move. If there is ataxia, a fracture of the body of the thoracic spine should be ruled out. Reasonable radiographs can be obtained of the majority of the bodies of the thoracic spines by using a technique for imaging the lungs. The air in the lungs produce a good contrast. Typically, the fractures would be compressive, so each segment needs to be measured to see if they are shorter in length.
Treatment of the fractures of the summits of the spine should be conservative. Exploration of the fracture hematoma and removal of the fracture pieces is not indicated and often can lead to chronic infections and, in one very notable case, a descending infection into the spinal canal.
Lumbar Spine Fracture
The lumbar spine (often the TL junction) can suffer catastrophic trauma, especially if the animal has been traveling at a high velocity and trips and then summersaults and lands on the lumbar area. The majority of horses are unable to rise, and many are found dead in a pasture a short distance from some object. It is important to recognize that a fracture in this area is a possibility and not subject the patient to the long process of dragging into an ambulance, transportation to hospital, and possible slinging. Spinal fluid from a lumbosacral tap may be normal or bloody. Subarachnoid corticosteroids could be injected in an attempt to reduce swelling. The prognosis is very unfavorable.
Sacrum/Coccygeal Fracture
Fracture is this area can occur from falling and sitting on their haunches, falling off one side on hard pavement, or from stress fractures in young racehorses. These are painful injuries, and many patients show bizarre behavior, often kicking out when moved or trying to run away from what seems to them to be a very noxious stimulus when the fracture fragments move. They often have at least Grade 2/5 ataxia behavior. The most consistent neurological deficit is that of a cauda equina syndrome with an inability to defecate and micturate (often the bladder is overflowing, and the urine dribbles out) and a very weak and flaccid tail. These clinical signs are very similar to the neurological form of herpes, and there can be some initial problems in sorting out the diagnosis. A rectal exam should be performed, not only to evacuate the rectum, but also to check for rectal tone and to palpate the bladder and manually assist in the emptying of it. While doing the rectal, the examiner should turn the palm dorsally to palpate for a firm enlargement on the ventral aspect of the sacrum. If this is suspected, a rectal ultrasound exam assists in determining the character of the enlargement. If it is a fracture, the surface of the bone will not be smooth, and the fluid will have the character of blood. A nuclear image with increased isotope uptake is very useful in confirming trauma as the most likely cause of neurological deficits. Fluid from a lumbosacral tap can be normal or xanthochromic.
Treatment consists of anti-inflammatory medication, stall restriction, sedation if showing violent activity when moving, evacuation of the rectum, and drainage of the bladder 4 times a day. The clinical signs can persist for 6 to 8 months. Epidural steroids are also indicated and can be repeated 2 to 3 times.
Spinal Stenosis
Many young, middle-aged, and older performance horses have either one or both articular facets of the caudal vertebra (C6/C7 is the most common) enlarged, often from a developmental problem (OCD), but can also have had a fracture. They can perform well for years, but suddenly, a traumatic incident (falling, pulling back) will be the straw that breaks the camel's back. The degree of ataxic behavior depends on the extent of the pathology.
A complete neurological exam will often show that the signs are more obvious on one side. Standing radiographs will show an enlarged facet, and an ultrasound exam will also demonstrate an enlarged facet with a roughened surface. Using ultrasound to guide a needle to administer intra-articular steroids can be done to reduce the swelling of the inflamed joint capsule that is putting pressure on the spinal cord. Many horses show dramatic results and can perform soon after. The owners, trainers, and riders need to be informed. If the degree of ataxia is Grade 2/5 plus, we recommend a myelogram before intra-articular therapy as a more accurate diagnosis and prognosis can be given. If there is dramatic cord compression, an anterior interbody fusion is indicated.
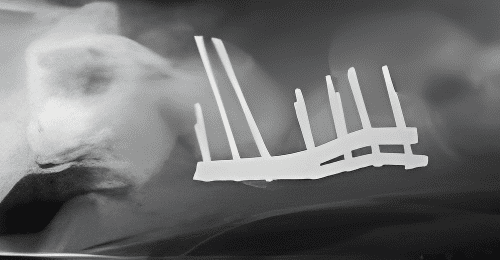
Fracture
Cervical Fracture of C4-5